

Article
Related Links
Hiroshi Fujita1*, Junji Tomiyama2, Shigeko Nishimura1
¹ Department of Transfusion Medicine, Tokyo Metropolitan Bokutoh Hospital, Tokyo, Japan
² Department of Internal Medicine, Tokyo Metropolitan Bokutoh Hospital, Tokyo, Japan
Abstract
Cardiac tamponade following sternal puncture is fatal and is caused by an anomaly such as foramen sterni, fragility of the bone, or high pressure exerted by doctors on the bone. Contact pressure associated with bone marrow aspiration is unknown; therefore, we examined the contact pressure resulting from bone marrow puncture for aspiration. Prescale, a pressure-sensitive film, was used for measurements. Contact pressure on wood surface at 2 heights, the knee and hip positions of the hematologists, was examined and was approximately 15 – 21 megapascals. The magnitude of the con-tact pressure did not change with the type of puncture needle. However, the contact pressure in the needle area at the hip position was higher than that at the knee position height, when doctors aspirated the bone marrow. Contact pressure resulting from bone marrow puncture was found to be high; therefore, hematologists should be aware of this force when dealing with patients.
Keywords: Bone Marrow Aspiration; Cardiac Tamponade; Contact Pressure; Iatrogenic Accident
1. Introduction
Cardiac tamponade following sternal puncture is usually fatal and is caused by 3 mechanisms, namely, an abnor-mality such as foramen sterni, fragility of the bone itself, or high pressure exerted by doctors on the bone [1,2]. Foramen sterni is often present in the sternal body at the 4th – 5th intercostal position, and its frequency of inci-dence in the general population is approximately 2% – 8% [3,4]. M. Inoue et al. reported that an anterior chest approach to sternal bone marrow aspiration involves a risk of laceration of the ascending aorta when the needle penetrates the sternum [5]. Mispuncturing at an inade-quate place might lead to an iatrogenic accident such as cardiac tamponade or aortic rupture [6]. We have previ-ously reported the irregularity and decreased bone den-sity of sternal bodies in patients with multiple myeloma [4]. If the pressure of bone marrow puncture is extremely strong, the needle may easily penetrate fragile sternal bodies. However, no studies have investigated this problem.
Fuji pressure-sensitive films (Fujifilm Co., Tokyo, Japan) have been widely used for studying contact mechanics in artificial joints and hand power [7-10]. The film is usu-ally composed of 2 polyurethane composite films, a microcapsule layer, and a color-developing layer. Five grades of Fujifilm are available, each covering a specific pressure range. Therefore, given that nothing was re-ported on this topic, we examined the contact pressure resulting from bone marrow puncture by using a Fuji pressure-sensitive film in order to obtain the information that may be useful for improving the medical safety dur-ing the procedure.
2. Methods
The Fuji pressure-sensitive film was purchased from Fu-jifilm Co. Two kinds of needles for bone marrow punc-ture were purchased from CareFusion Japan (DIN1518X, 15 G; Tokyo, Japan) and TSK Laboratory (SIL-151, 15 G; Tochigi, Japan).
For the assessment of the Fuji pressure-sensitive film on the surface of cork board (Kawai Woodworking Co., Tokyo, Japan), bone marrow puncture was performed by hematologists with at least 10 years of experience. We examined the contact pressure on the wood surface at 2 heights, at the knee and hip positions of the hematologists.
For contact pressure measurements, we used the Fuji Prescale medium grade pressure film with a pressure range of 10 – 50 megapascals (MPa) and an operating temperature range of 20°C – 28°C [7,8]. The average am-bient room temperature during the trials was approxi-mately 23°C under dry test conditions. Each Fujifilm patch result was scanned using a Prescale Data Shot FPD-100 (Fujifilm Co.). The contact patch scans were analyzed using Prescale pressure imaging and analysis software, FPD-100S version 1.0 (Fujifilm Co.) to quan-tify the total contact area.
We compared the differences between the 2 groups (i.e., knee position vs hip position, or needle area vs stopper area) using the Wilcoxon signed-rank test. Data were expressed as mean ± standard error of mean values for the groups. All statistical procedures were conducted using JMP version 8.0 software (SAS Institute, Inc., Cary, NC, USA), and significance was set at P < 0.05.
3. Results
We measured the contact pressures of both the needle and stopper areas when hematologists used the bone marrow aspiration needle (CareFusion Japan); the results are shown in Table 1 and Figure 1.

Figure 1. (a) Bone marrow aspiration needle: In this paper, we used two kinds of needles for bone marrow puncture pur-chased from CareFusion Japan (DIN1518X, 15 G; Tokyo, Japan) and TSK Laboratory (SIL-151, 15 G; Tochigi, Japan). He-matologists (Table 1) performed the bone marrow puncture on wood using a needle purchased from CareFusion Japan, as shown in (a); (b) Pressure sensitive film showing the contact pressure from bone marrow puncture: The Fuji Prescale medium grade pressure-sensitive film with a pressure range of 10 – 50 MPa was used for measuring contact pressure. Hematologist #2 (Table 1) performed the bone marrow puncture on wood using a needle purchased from CareFusion Japan (a). Contact pressure changed the color on the prescale film from the white to pink, or red color dependent on the grade of pressure. Pressure changes were noted at the needle area (center position) and at the stopper area (around the needle area).
The contact pressure in the needle area at the hip posi-tion was 15.2 – 21.4 MPa, which was significantly higher than the contact pressure recorded in the stopper area (7.2 – 11.1 MPa). Similar results were found for the con-tact pressure at the knee position. As shown in Table 1, hematologist #2 also performed the bone marrow punc-ture using a needle purchased from TSK Laboratory (contact pressure of the CareFusion needle: 21.4 ± 0.5 MPa; contact pressure of the TSK Laboratory needle: 21.1 ± 0.9 MPa, N = 10). After 3 months, hematologist #2 performed the puncture experiments again and the contact pressure in the needle area resulting from bone marrow puncture at the hip position had reduced com-pared with the first readings (18.9 ± 1.5 MPa, N = 10).
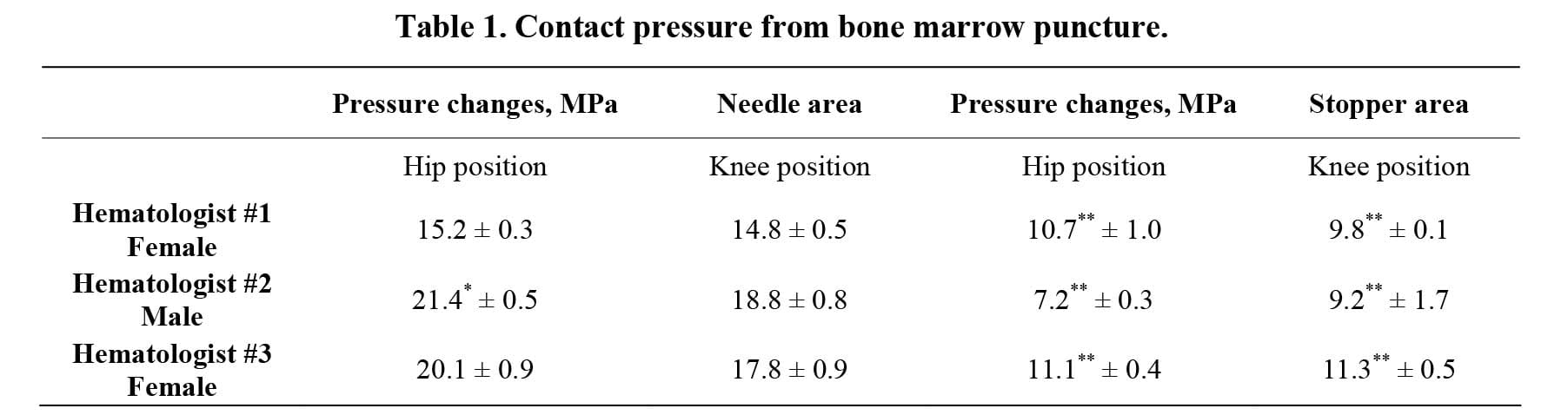
Each hematologis
t performed the bone marrow puncture on wood 10 times using a needle purchased from CareFusion Japan at both the hip and knee positions. Data are presented as mean and standard error of mean values. *P < 0.05 vs. knee position, **P < 0.05 vs. needle pressure.
4. Discussion
No papers on contact pressure from bone marrow punc-ture have been published previously. First, we reported that the contact pressure from bone marrow puncture ranges from approximately 15 MPa to 21 MPa (15 – 21 N/mm2 or 150 – 210 kg/cm2), as shown in Table 1. Sev-eral reports have been published on pressure studies of artificial joints for other medical procedures, using Fuji pressure-sensitive films [7,8]. For example, contact pressure for the knee joint from 1115 N at 20°C was de-termined to be approximately 7.3 MPa [7]. Therefore, the contact pressure resulting from bone marrow puncture performed by hematologists was stronger than that at the knee joint in artificial joint experiments. On the other hand, Liau et al. suggested that Fuji pressure-sensitive film might overestimate contact pressure compared with other measurements [9]. Moreover, in this study, the measurement of contact pressure was made on wood, not on human bodies, which may be a limitation.
Despite this, attention should be paid to the force used during bone marrow aspiration because of the high con-tact pressure involved, and particularly in patients with multiple myeloma, which is a hematological malignancy associated with bone fragility [4,10]. High pressure re-sulting from bone marrow puncture may also induce sternal destruction, resulting in cardiac tamponade. When hematologist #2 repeated the puncture experiments, the contact pressure decreased from 21.4 MPa to 18.9 MPa, suggesting that the degree of force used during bone marrow aspiration might reduce the contact pressure. Three hematologists exerted higher pressure at the hip position than at the knee position. We speculate that it is easier to apply pressure from a lumbar height than at the knee level. The difference in contact pressure resulting from bone marrow puncture at the position of patients from the viewpoint of the performer (i.e., the hematolo-gists) should also be considered. In conclusion, we be-lieve that the information on contact pressure reported in this paper will be useful for improving medical safety during bone marrow aspiration.
5. Acknowledgments
This study was supported by a grant from Tokyo Metro-politan Government.
References
- B. L. Bhootra, “Fatality Following a Sternal Bone Mar-row Aspiration Procedure: A Case Report,” Medicine, Science and the Law, Vol. 44, No. 2, 2004, pp. 170-172. doi:10.1258/rsmmsl.44.2.170
- R. J. Van Marum and L. te Velde, “Cardiac Tamponade Following Sternal Puncture in Two Patients,” The Neth-erlands Journal of Medicine, Vol. 59, No. 1, 2001, pp. 39-40. doi:10.1016/S0300-2977(01)00126-7
- E. Yekeler, M. Tunaci, A. Tunaci, M. Dursun and G. Acunas, “Frequency of Sternal Variations and Anomalies Evaluated by MDCT,” American Journal of Roentgenol-ogy, Vol. 186, No. 4, 2006, pp. 956-960.doi:10.2214/AJR.04.1779
- H. Fujita, S. Nishimura and K. Oyama, “Retrospective Study on CT Findings of the Sternal Bone after Bone Marrow Aspiration Procedure in Hematological Patients (Japanese),” The Japanese Journal of Clinical Hematol-ogy, Vol. 50, No. 12, 2009, pp. 1687-1691.
- M. Inoue, T. Nakasato, K. Yamauchi, Y. Nakamura, S. Oshida and S. Ehara, “Risk Factors Concerning Sternal Bone Marrow Aspiration and Patient Safety in Japan,” Internal Medicine, Vol. 49, No. 12, 2010, pp. 1089-1095.
- T. B. Halvorsen, S. S. Anda, A. B. Naess and O. W. Le-vang, “Fatal Cardiac Tamponade after Acupuncture through Congenital Sternal Foramen,” The Lancet, Vol. 345, No. 8958, 1995, p. 1175.doi:10.1016/S0140-6736(95)91004-2
- R. Zdero, P. V. Fenton, J. Rudan and J. T. Bryant, “Fuji Film and Ultrasound Measurement of Total Knee Arthro-plasty Contact Areas,” The Journal of Arthroplasty, Vol. 16, No. 3, 2001, pp. 367-375.doi:10.1054/arth.2001.21501
- Y. Nakagawa, “Measuring Perineum Pressure through Midwife’s Hand during Shoulder Delivery (Japanese),” Journal of Japan Academy of Midwifery, Vol. 19, No. 1, 2005, pp. 30-42.doi:10.3418/jjam.19.1_30
- J.-J. Liau, C.-C. Hu, C.-K. Cheng, C.-H. Huang and W.-H. Lo, “The Influence of Inserting a Fuji Sensitive Film be-tween the Tibiofemoral Joint of Knee Prosthesis on Ac-tual Contact Characteristics,” Clinical Biomechanics, Vol. 16, No. 2, 2001, pp.160-166.doi:10.1016/S0268-0033(00)00040-1
- M. T. Drake, “Bone Disease in Multiple Myeloma,” On-cology, Vol. 23, No. 14, 2009, pp. 28-32.
![]()