

Article
Related Links
Katie McLellan, Ph.D., Jerrold S. Petrofsky, Ph.D., J.D., Grenith Zimmerman, Ph.D., Everett Lohman, D.Sc., P.T., Michelle Prowse, M.S., P.T., Ernie Schwab, Ph.D., and Scott Lee, M.D.
Abstract
Background: To protect against ischemia, pressure-induced vasodilation (PIV) causes an increase in skin blood flow. Endothelial dysfunction, which is commonly found in older patients and those with diabetes, and global temperatures can affect the resting blood flow in skin, which may reduce the blood flow during and after the application of local pressure. The present study investigated the PIV of the skin with exposure to three global temperatures in younger and older populations and those with diabetes.
Materials and Methods: Older subjects (n=15, mean age 64.2±14.0 years), subjects with diabetes (n=15, mean age 62±5.9 years, mean duration 13.2±9.1 years), or younger subjects (n=15, mean age 25.7±2.9 years) participated. An infared laser Dopler flow meter was used to measure skin blood flow on the bottom of the foot, lower back, and hand during and after applications of pressure at 7.5, 15, 30, 45, and 60 kPa at 16°C, 24°C, and 32°C global temperatures.
Results: The resting blood flow for all subjects was significantly lower in the 16°C environment (P<0.05). Blood flow in the group with diabetes was significantly lower at rest, during the application of all pressure, and after the release of pressure in all global temperatures (P<0.05). The younger group showed a significant increase in blood flow after every pressure application, except 7.5 kPa, in all global conditions (P<0.001). Older subjects and patients with diabetes did not have a significant reactive hyperemia, especially in the 16°C environment.
Conclusions: The protective mechanism of PIV is severely reduced in older populations and those with diabetes, especially in colder environments where skin blood flow is already diminished.
Introduction
When pressure is applied to the skin, affected tissues can become hypoxic and build up levels of vasodilator metabolites, which dilate the arterioles and decrease the vascular resistance in healthy skin.1 Once the pressure is released, local blood flow is temporarily elevated because of the reduced vascular resistance. The temporary increase in blood flow is called a reactive hyperemia, which serves to reoxygenate the tissue and flush the vasodilator metabolites from the tissue.2
The ability of the skin to protect itself from anoxia during ischemia can be diminished due to endothelial dysfunction.3 This type of vascular dysfunction can diminish the degree of vasodilation associated with a reactive hyperemia. Endothelial dysfunction is an early event and associated with a host of diseases and conditions, such as aging and diabetes. The prognostic value of endothelial dysfunction is just starting to be understood and valued. One way of noninvasively assessing endothelial dysfunction is by looking at endothelium-dependent vasodilation.4
One major factor of endothelium-dependent vasodilation is nitric oxide (NO).2,5 NO is released by the endothelium in response to exogenous pharmacological substances, plateletderived factors, and shear stress, which promote the release of NO by stimulating NO synthase.2,6,7 The NO then causes the smooth muscle surrounding the blood vessel to relax, causing it to vasodilate. Local pressure also causes a temporary increase in blood flow, known as a pressure-induced vasodilation (PIV), which causes a subsequent release of NO.8 PIV is a natural protective mechanism, allowing the skin blood flow to increase temporarily after local pressure is applied.9,10
Endothelial dysfunction can reduce the body’s ability to produce and=or respond to NO.4 With damage to the vascular endothelial cells, such as is common in older people,11 the microcirculation of the skin may not be able to respond to endothelial stressors such as pressure or global temperature.3,12,13 Preliminary data from this laboratory have shown decreased endothelial responses to multiple stressors, especially in people with diabetes.13–17
Diabetes is an increasingly common disease, with an incidence of at least 10% in the United States, and it has been predicted to reach as high as 30% of the world’s population by the year 2025.18 Of all the complications associated with diabetes, the most common is damage to the microcirculation and endothelial cells.19 This vascular endothelial damage results in a reduced ability either to produce NO or a reduced sensitivity to NO.20,21
Age can also be a factor that may reduce the protective response of PIV. As humans age, the endothelial cells undergo the same type of damage as a person with diabetes: reduced sensitivity to or less NO released in response to external stimuli.13–15,22 Prior studies indicate there may be a decrease in skin blood flow when low pressures are applied to the skin in patients with diabetes both with and without neuropathies, compared to control subjects.10,23–25 Therefore, a more comprehensive study needs to be done to examine the PIV of subjects with and without diabetes with multiple endothelial stressors.
Changes in global temperature alter resting blood flow in the skin.13,26 People live in a variety of global temperatures, and previous studies on pressure effects on skin blood flow had been on subjects who are young and people without diabetes in a thermally neutral room. Thus these studies do not examine most people under normal environmental conditions. Therefore, the purpose of the present study was to investigate the effects of global temperatures on endothelial dysfunction by repeating the series in thermally neutral, cool, and warm climates to examine the effects of resting blood flow on PIV on subjects who were older and who had diabetes. The aim was also to expand upon previous research by examining the reactive hyperemia following local pressure on the foot compared to the lower back and hand. We hypothesize that subjects who are older and with diabetes will have a reduced PIV response due to endothelial damage, compared to age-matched subjects with diabetes and younger subjects. We also hypothesize that the reactive hyperemia associated with PIV will be decreased in a colder environment when compared to the response in a warmer environment. The damaged endothelial cells and adjacent microcirculation may experience diminished PIV in response to local pressure. Therefore, three groups of subjects were investigated: a younger group without diabetes and an older group, age-matched to an older group with type 2 diabetes.
Subjects and Methods
Subjects
A total
of 45 subjects (three groups, 15 subjects each) participated (Table 1). The subjects with diabetes must have been diagnosed with diabetes at least 3 years ago, been taking the proper medication to control their blood sugar levels, and have hemoglobin A1c levels between 6% and 10%. Subjects were excluded if they had any current or past heart problems or high blood pressure (>140mm Hg systolic=95mm Hg diastolic) or were taking any α- or β-agonists or antagonists. All protocols and procedures were approved by the Institutional Review Board at Loma Linda University, Loma Linda, CA, and subjects signed an informed consent document.
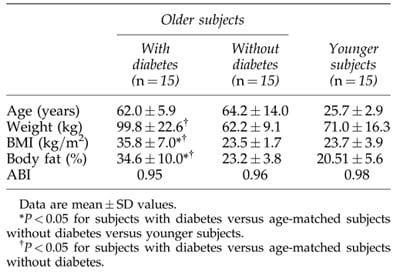
Table 1. Clinical Characteristics of 30 Age-Matched Older Subjects (Half with Diabetes) and 15 Younger Subjects
There was a significant difference in the body mass index (BMI) among all three groups (P<0.001) (Table 1), with the subjects with diabetes having the highest overall BMIs. There was no significant difference between the mean ages for the older group and the group with diabetes (P=0.58). In terms of the ankle-brachial index (ABI), none of the 45 subjects had an ABI score lower than 0.95. The subjects with diabetes had a mean hemoglobin A1c of 7.6±1.1% and had been diagnosed for a mean of 13.2±6.1 years.
Control of environmental temperature
Environmental temperature was controlled using a controlled environment room. The room has thermal homogeneity (laminar flow) with air flow maintained with independent heating and cooling systems capable of controlling room temperature over a range from 0°C to 55°C. The application of two independent heating and cooling systems allows rapid changes in room temperature, up to 7°C/min, and the environmental temperature to be accurately controlled to within ±0.5°C. Three room temperatures were used: 16°C, 24°C, and 32°C. Relative humidity was maintained at 35±10%.
Measurement of pressure on the skin
Pressure on the skin was measured through a pressure sensor array (Tactilus Pressure Mapping System, Sensor Products Inc., Madison, NJ), which contained about 500 sensors. The pressure sensors were 7.94×7.94mm and were spaced in intervals of 44.5×4.5mm. The thickness of the sensor was 7mm. The sensor used was a resisted strain gauge sensor produced by Sensor Products Inc. The pressure range was 0–68 kPa. The accuracy and reliability were less than 3% error. Calibration was done at the factory as well as randomly throughout the study. The system and software were custom designed for this project to provide a three-dimensional map of pressure distribution. The array was transduced through a 16-bit A/D converter produced by Sensor Products Inc. with a sample rate of 100 KHz. The three skin sites were the back of the hand between the second and third metacarpal, the lower back 7 cm lateral of the L3–L4 vertebrae, and over the head of the first metatarsal on the ball of the foot.
Measurement of blood flow
A single-point infrared laser Doppler flow meter (TST 140 probe, LDF100 module, Biopac Inc., Goleta, CA) was used to measure the skin blood flow. The skin blood flow was recorded for 30s. The flow meter had a head with an active area of 1cm2. The probe was plugged into an LDF 100C amplifier and then digitized at 2,000 samples per second with a 16-bit analog to digital converter. The converted signal was then saved for final analysis with a Biopac MP 100 system (Biopac).
Measurement of ABI Blood pressure measurements were taken at the ankle and brachial artery in the arm using a standard sphygmomanometer cuff and stethoscope while the subject was at rest and had been lying supine for at least 5 min. The ankle and arm systolic blood pressure measurements for the left and right limbs were recorded. The ABI is derived by dividing the systolic pressure of the ankle by the systolic pressure of the brachial artery, and the result is used to predict the severity of peripheral arterial disease. The ABI range that is generally considered normal is 0.95–1.2.
Total body fat percentage
The total body fat percentage was measured by an impedance plethysmograph (RJL Systems, Clinton Twp., MI). The Quantum II provides high-resolution whole body and regional bioelectrical resistance and reactance measurements. The total body fat percentage was measured through electrodes placed on the right foot and right hand.
Procedures
On three different days, the subjects sat comfortably in the controlled environment roomat 16°C, 24°C, or 32°C for 20 min. Before any pressure was applied, the baseline blood flow was taken. The laser Doppler flow probe was placed on the ball of the foot. The pressure array was placed on top of the probe, and manual pressure was applied for 30s while the blood flow was recorded. The pressure was removed for 30s, and recording of the blood flow continued. Pressure was applied in a random order at 7.5, 15, 30, 45, and 60 kPa. These steps were repeated on the lower back and the back of the hand.
Statistics
Calculations of means and SDs were done, and all results are expressed as mean ±SD values. Comparisons among groups were performed using one-way analysis of variance and independent t tests. The level of significance was P≤0.05. The results were analyzed using SPSS version 15 (SPSS, Chicago, IL).
Results
Three temperatures were examined; first, a neutral global temperature, then a warm temperature, and, finally, a cold global temperature.
24°C global temperature
Application of pressure. In the thermally neutral global temperature (24°C), when pressure was applied for 30s, the blood flow to the skin of the foot on the younger subjects decreased proportionally to the amount of pressure being applied (Fig. 1). The subjects who had diabetes had a significant decrease in blood flow from the lowest pressure used in this study (7.5 kPa) compared to baseline blood flows (POlder=0.04, PDiabetes=0.03). When the greatest pressure used in this study (60 kPa) was applied to the foot, the younger subjects had a blood flow of 17.48±2.63 flux, which was significantly higher than the subjects who were older (9.52±1.41 flux, P=0.02) and with diabetes (4.72±0.67 flux, P<0.05). The pattern of response was similar for the hand and lower back.
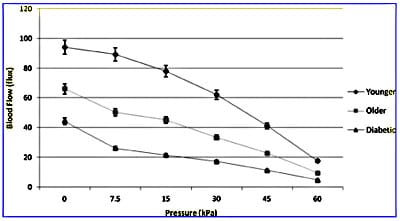
Fig. 1. Vascular occlusion on the foot due to application of 30s of pressure in three groups of subjects in 24°C global temperature with standard deviation error bars.
Blood flow after application of pressure.
The reactive hyperemia following the application of very light pressure (7.5 kPa) on the foot resulted in a significant increase in blood flow for the younger subjects (P=0.03), but not for the subjects who were older with or without diabetes (Fig. 2). On the lower back and hand, the responses were similar. For the applications of 15, 30, 45, and 60 kPa on the foot, there was no significant difference between the PIV for the older subjects and the subjects with diabetes. When the PIV of the foot and hand were compared, there was no significant difference in the PIV at baseline or for any of the pressure applications. However, the lower back had significantly lower blood flow responses (P=0.02). Figure 3 shows a comparison of the blood flow at baseline, 30 kPa, and 60 kPa for the lower back and foot.
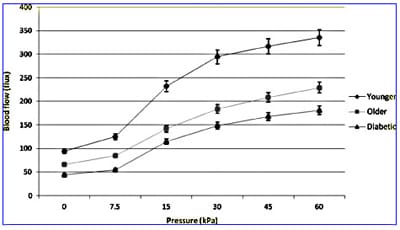
Fig. 2. PIV of the foot due to application of 30s of pressure for three groups of subjects in 24°C global temperature with standard deviation error bars.
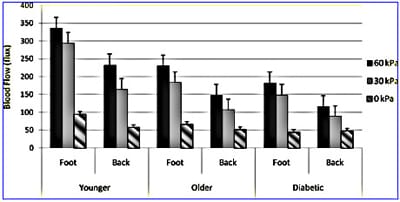
Fig. 3. Blood flow in the skin at different pressures on the foot and lower back for three groups of subjects in 24°C global temperature with standard deviation error bars.
32°C global temperature
Application of pressure. In the warmer environment, 30s of pressure resulted in similarly occluded blood flow as in the 24°C global temperature for the foot, hand, and back. There was a significant increase in resting blood flow for the foot (P=0.02) and hand (P=0.04), but not the back (P=0.17) for all subjects. The lower back did not have a significant increase in resting blood flow (P=0.17) or PIV from any amount of pressure (P=0.36). The blood flow response of heavy pressure (60 kPa) on the foot significantly increased blood flow in the 24°C compared to the 32°C global temperatures (P=0.02) with increases of 27.6% for the younger subjects, 30.3% for the older subjects, and 22.5% for the subjects with diabetes (Fig. 4). For all other applications of pressure on the foot, there was no significant increase in blood flow from the 24°C global temperature to the 32°C global temperature for any of the groups of subjects. The response was similar for the hand.
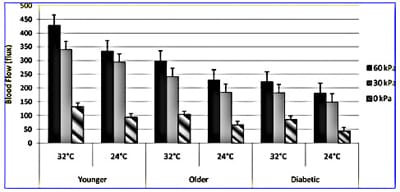
Fig. 4. Comparison of PIV of the foot due to application of 30s of pressure for three groups of subjects in 32°C and 24°C global temperatures with standard deviation error bars.
16°C global temperature
Application of pressure. The occlusion resulting from each application of pressure is displayed in Figure 5 for the foot for each group of subjects. For the subjects with diabetes, there was no significant difference between baseline blood flow and the occluded blood flow due to 30s of any of the applications of pressure. The pattern of response was similar for the lower back and hand.
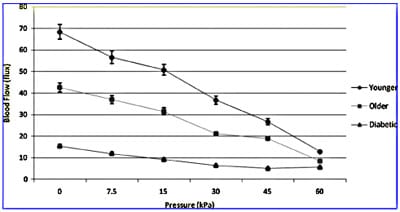
Fig. 5. Vascular occlusion on the foot due to application of 30s of pressure in three groups of subjects in 16°C global temperature with standard deviation error bars.
The baseline blood flow of the foot for the subjects with diabetes was 15.42±3.26 flux, which was 276% lower than for the older subjects and 443% lower than the blood flow of the younger subjects. This difference in blood flows between the three groups of subjects was statistically significant (P=0.01). The pattern of PIV response to the various amounts of pressure application was similar in the 16°C and 24°C global temperatures. Results were similar for the lower back and hand.
Comparison of the three groups of subjects
When the PIV for each application of pressure was compared to the baseline blood flow in the 16°C global temperature, the subjects with diabetes had significantly higher increases in blood flow compared to the age-matched subjects without diabetes (P=0.01) (Fig. 6). At the 24°C global temperature, the subjects with diabetes had a larger percentage increase in blood flow from baseline than the older subjects for all of the pressure applications except 7.5kPa. The 32°C global temperature did not cause the blood flow to increase more in the subjects with diabetes than the older subjects without diabetes for any application of pressure. The differences were not significant for the blood flow and percentage blood flow increases for the subjects who were older compared to the subjects with diabetes.
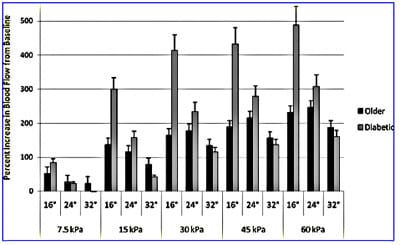
Fig. 6. Percentage increase in blood flow from baseline of older age-matched subjects with and without for all pressure amounts in three global temperatures with standard deviation error bars.
Discussion
When pressure is applied to the skin, blood flow is temporarily reduced or occluded. Once pressure is released, the PIV occurs to reoxygenate the skin and tissues through briefly vasodilated skin blood flow.1 Endothelial dysfunction, such as is common in people who are older or who have diabetes, 4,13,26 may reduce the PIV blood flow,3,9,10 and affected tissues may not be reoxygenated properly. The vascular endothelial cells may be stressed by changes in global temperatures, which may further reduce the reactive hyperemia associated with PIV.3,13
In the present investigation, for the younger subjects, the pattern of response of pressure versus blood flow was similar after exposure to all three global temperatures. Overall, the pattern of response of the decreased blood flow was similar for the foot, lower back, and hand. For the PIV, in the 24°C and 32°C environments, the slope of the lines of the subjects who were older and who had diabetes were nearly parallel. The subjects with diabetes had a blood flow response that was a mean of 29 flux lower in the 24°C and 51 flux lower in the 32°C global temperature than the older subjects. In the 16°C environment, the pattern of response was similar for the older and younger subjects; however, the subjects with diabetes had a blood flow response that was significantly lower than the younger and older subjects for all applications of pressure, except 60kPa. The foot and hand had similar PIV responses, whereas the lower back had a similar pattern but an overall reduced blood flow by a mean of 50 flux. Although the baseline blood flow for the subjects with diabetes was significantly lower in the 16°C and 24°C global temperatures, they had a larger percentage increase in blood flow as a result of the 15, 30, 45, and 60kPa applications of pressure than the age-matched older subjects without diabetes. This suggests that local pressure may help to cause temporary increases in blood flow, which may be useful in therapy and treatment plans for populations with diabetes.
Previous studies from this laboratory have shown the responses of vascular endothelial cells to stimuli, such as global temperature or pressure, are affected by stimuli from their environment.3,13–16,27,28 Similar to data presented here, skin blood flow was decreased at low pressure applications in subjects with diabetes,9 which indicates an inability of the skin to respond to small amounts of stress to the microcirculation and endothelial cells. Chronic pressure applications have been shown to further reduce the PIV mechanism in patients with diabetes, suggesting C-fibers are involved in cutaneous vasodilation.9 Three main biochemical pathways may decrease NO availability and increase endothelial dysfunction: the polyol pathway, nonenzyme glycation, and redox potential alterations.24,29 NO production can be impaired by increa
sed flux of the polyol pathway, which can completely decrease NADPH.30–34 Advanced glycation end product accumulation reducesNObioavailability24,29 and has been seen in early stages of diabetes,35 which suggests endothelial alterations had already started.
Global and skin temperatures may also play an important role in determining the magnitude of PIV. The present data show the colder environment resulted in significantly reduced blood flow due to pressure applications and PIV once the pressure was removed for all groups of subjects. This suggests PIV mechanisms may be receptive to mechanothermal nervous receptors as well as biomechanical pressure.10 A recent study from this lab showed vasodilation was attenuated in skin that had been both locally and globally heated.36 These data are similar to those of people with type 1 diabetes in whom an impaired skin blood flow response to pressure was also seen.37 In this study, NO product was also impaired in people with type 1 diabetes.
Conclusions
The PIV mechanism was reduced in the colder 16°C global temperature in the older subjects without diabetes and, most significantly, in the subjects with diabetes regardless of the environmental temperature. The PIV response seems to be highly sensitive to endothelial NO levels. Older people and people with diabetes may have damaged endothelial cells, causing this response to be absent or diminished. PIV could be a noninvasive indicator of endothelial dysfunction that can be used to diagnose patients that may be predisposed to microvascular problems such as pressure ulcers.
Limitations
One of the limitations of this study is that we did not apply pressure less than 7.5 kPa. It is possible that people with diabetes will have a reactive hyperemia to lighter forces of pressure such as 3 kPa, but that was not examined in this study.
Acknowledgments
The authors thank Anshul Sharma for technical assistance.
Author Disclosure Statement
No competing financial interests exist.
REFERENCES
- Wilkin JK: Cutaneous reactive hyperemia: viscoelasticity determines response. J Invest Dermatol 1987;89:197–200.
- Minson CT, Berry LT, Joyner MJ: Nitric oxide and neutrally mediated regulation of skin blood flow during local heating. J Appl Physiol 2001;91:1619–1629.
- Petrofsky JS, Bains GS, Prowse M, McLellan K, Ethiraju G, Lee S, Gunda S, Lohman E, Schwab E: The influence of age and diabetes on the skin blood flow response to local pressure. Med Sci Monit 2009;15:CR325–CR331.
- Endemann D, Schiffrin E: Endothelial dysfunction. J Am Soc Nephrol 2004;15:1983–1992.
- Smits P, Williams SB, Lipson DE, Banitt P, Rongen GA, Creager MA: Endothelial release of nitric oxide contributes to the vasodilator effect of adenosine in humans. Circulation 1995;92:2135–2141.
- Dudzinski DM, Igarashi J, Greif D, Michel T: The regulation and pharmacology of endothelial nitric oxide synthase. Ann Biomed Eng 2006;46:235–276.
- Mombouli JV, Vanhoutte PM: Endothelial dysfunction: from physiology to therapy. J Mol Cell Cardiol 1999;31: 61–74.
- Garry A, Sigaudo-Roussel D, Merzeau S, Odile D, Saumet JL, Fromy B: Cellular mechanisms underlying cutaneous pressure-induced vasodilation: in vivo involvement of potassium channels. Am J Physiol Heart Circ Physiol 2005; 289:H174–H180.
- Fromy B, Merzeau S, Abrahan P, Saumet JL: Mechanisms of the cutaneous vasodilator response to local external pressure application in rats: involvement of the CGRP, neurokinins, prostaglandins and NO. Br J Pharmacol 2000;131:1161– 1171.
- Fromy B, Abraham P, Bouvet C, Bouhanic B, Fressinaud P, Soumet JL: Early decrease of skin blood flow in response to locally applied pressure in diabetic subjects. Diabetes 2002;51:1214–1217.
- Holowatz LA, Thompson CS, Minson CT, Kenney WL: Mechanisms of acetylcholine-mediated vasodilation in young and aged human skin. J Physiol 2005;563:965–973.
- Medeiros JV, Gadelha GG, Lima SJ, Garcia JA, Soares PM, Santos AA, Brito GA, Ribeiro RA, Souza MH: Role of the NO=cGMP=KATP pathway in the protective effects of sildenafil against ethanol-induced gastric damage in rats. Br J Pharmacol 2008;153:721–727.
- Petrofsky J, Lohman E 3rd, Lee S, De la Cuesta Z, Labial L, Iouciulescu R, Moseley B, Korson R, Al Malty A: Effects of contrast baths on skin blood flow on the dorsal and plantar foot in people with type 2 diabetes and age-matched controls. Physiother Theory Pract 2007;23:189–197.
- Petrofsky JS, Lee S, Cuneo-Librona M: The impact of rosiglitazone on heat tolerance in patients with type 2 diabetes. Med Sci Monit 2005;11:CR562–CR569.
- Petrofsky JS, Lee S, Patterson C, Cole M, Stewart B: Sweat production during global heating and during isometric exercise in people with diabetes. Med Sci Monit 2005;11: CR515–CR517.
- Petrofsky J, Lee S, Cuneo-Librona M, Apodaca P: The effect of rosiglitazone on orthostatic tolerance during heat exposeure in individuals with type II diabetes. Diabetes Technol Ther 2007;9:377–386.
- Petrofsky JS, Al-Malty AM, Prowse M: Relationship between multiple stimuli and skin blood flow. Med Sci Monit 2008;14:CR399–CR405.
- Narayan V, Boyle JP, Thompson TJ, Sorenson SW, Williamson DF: Lifetime risk for diabetes mellitus in the United States. JAMA 2003;290:1884–1890.
- Rendell M, Bamisedun O: Skin blood flow and current perception in pentoxifylline-treated diabetic neuropathy. Angiology 1992;43:843–851.
- Hogikyan RV, Galecki AT, Pitt B, Halter JB, Greene DA, Supiano MA: Specific impairment of endotheliumdependent vasodilation in subjects with type 2 diabetes independent of obesity. J Clin Endocrinol Metab 1998;83: 1946–1951.
- Caballero AE, Arora S, Saouaf R, Lim SC, Smakowski P, Park JY, King GL, LoGerfo FW, Horton ES, Veves A: Microvascular and macrovascular reactivity is reduced in subjects at risk for type 2 diabetes. Diabetes 1999;48:1856–1862.
- Petrofksy JS, Lee S, Cuneo M: Effects of aging and type 2 diabetes on resting and post occlusive hyperemia of the forearm; the impact of rosiglitazone. BMC Endocr Disord 2005;5:4.
- Fromy B, Abraham P, Aumet JL: Non-nociceptive capsaisinsensitive nerve terminal stimulation allows for an original vasodilatory reflex in the human skin. Brain Res 1998;811: 166–168.
- Chan NN, Valance P, Colhoum HM: Nitric oxide and vascular responses in type I diabetes. Diabetologia 2000;43: 137–147.
- Peiper GM: Review of alteration in endothelial nitric oxide production in diabetes. Protective role of arginine on endothelial dysfunction. Hypertension 1998;31:1047–1060.
- Charkoudian K: Skin blood flow in adult human thermoregulation: how it works, when it does not, and why. Mayo Clinic Protocol 2003;78:603–612.
- Petrofsky JS, McLellan K, Bains G, Prowse M, Ethiraju G, Lee S, Gunda S, Lohman E 3rd, Schwab E: The influence of ageing on the ability of the skin to dissipate heat. Med Sci Monit 2009;15:CR261–CR268.
- Petrofsky JS, Bains G, Chinna R, Lohman E, Berk L, Prowse M, Gunda S, Madani P, Batt J: The effect of the moisture content of a local heat source on the blood flow response of the skin. Arch Dermatol Res 2009;301:581–585.
- Brownlee M: Biochemistry and molecular cell biology of diabetic complications. Nature 2001;414:813–820.
- Greene DA, Chakrabarti S, Lattimer SA, Sima AA: Role of sorbitol accumulation and myo-inositol depletion in paramodal swelling of large myelinated nerve fibers in the insulin-deficient spontaneously diabetic Bio-Breeding rat: reversal of insulin replacement, an aldose reductase inhibitor, and myo-inositol. J Clin Invest 1978;79:1479–1485.
- Soriano FG, Virag L, Jactap P,
Szabo E, Mabley JG, Liaudet L, Marton A, Hoyt DG, Murthy KGK, Salzman AL, Southan GJ, Szabo C: Diabetic endothelial dysfunction: the role of poly (ADP-ribose) polymerase activation. Nat Med 2001;7:108–113. - Stevens MJ, Dananberg J, Feldman EL, Lattimer SA, Kamijo M, Thomas TP, Shindo H, Sima AA, Greene DA: The linked roles of nitric oxide, aldose reductase, and (Naþ, Kþ)-ATPase in the slowing of nerve conduction in the streptozotocin diabetic rat. J Clin Invest 1994;94:853–859.
- Cameron NE, Cotter MA, Basso M, Hohman TC: Comparison of the effects of inhibitors of aldose reductase and sorbitol dehydrogenase on neurovascular function, nerve conduction and tissue polyol pathway metabolites in streptozotocininduced diabetic rats. Diabetologia 1997;40:271–281.
- Cameron NE, Cotter MA, Dines KC, Hohman TC: Reversal of defective peripheral nerve conduction velocity, nutritive endoneurial blood flow, and oxygenation by a novel aldose reductase inhibitor, WAY-121-509, in streptozotocininduced diabetic rats. J Diabetes Complications 1996;10: 43–53.
- Sigaudo-Roussel D, Demoit C, Fromy B, Koitka A, Leftheroitis G, Abraham P, Saumet JL: Early endothelial dysfunction severely impairs skin blood flow response to local pressure application in streptozotocin-induced diabetic mice. Diabetes 2004;53:1564–1569.
- McLellan K, Petrofsky JS, Zimmerman G, Prowse M, Bains G, Lee S: Multiple stressors and the response of the vascular endothelial cells; the effect of aging and diabetes. Med Eng Phys 2009;31:165–172.
- Koi¨tka A, Abraham P, Bouhanick B, Sigaudo-Roussel D, Demiot C, Saumet JL: Impaired pressure-induced vasodilation at the foot in young adults with type 1 diabetes. Diabetes 2004;53:721–725.
![]()